Transtracheal Wash
The transtracheal wash is performed in a sedated dog to obtain a fluid sample from the airway. This technique is helpful in patients that cannot undergo general anesthesia for a bronchoalveolar lavage and does not require a bronchoscope. The technique is lower yield compared to a bronchoalveolar lavage.
Summary of the Procedure:
| Indications | To obtain a sample from the trachea and larger lower airways for cytology and microbial culture in the work-up of the coughing animal.
Best to perform in medium to large breed dogs (difficult in small dogs / cats due to small diameter trachea) |
| Limitations | Limited value in animals with primary pulmonary parenchymal disease that are not coughing. |
| Complications | Uncommon.
Subcutaneous emphysema, pneumomediastinum, pneumothorax, airway bleeding, cellulitis. Inflammation may worsen, and dyspnea may occur, following an airway wash of any sort especially with eosinophilic bronchitis in dogs and asthma in cats. |
| Contraindications | Bleeding disorder, dyspnea. |
| Supplies/instruments | 12 in through-the-needle catheter.
12 mL syringe Sterile saline (#11 or #15 scalpel blade – optional) |
| Position | Sitting with head elevated and neck extended. |
| Restraint | Manual or mild sedation (avoid narcotics – they act as anti-tussives); local lidocaine block |
Landmarks (choose one or the other):
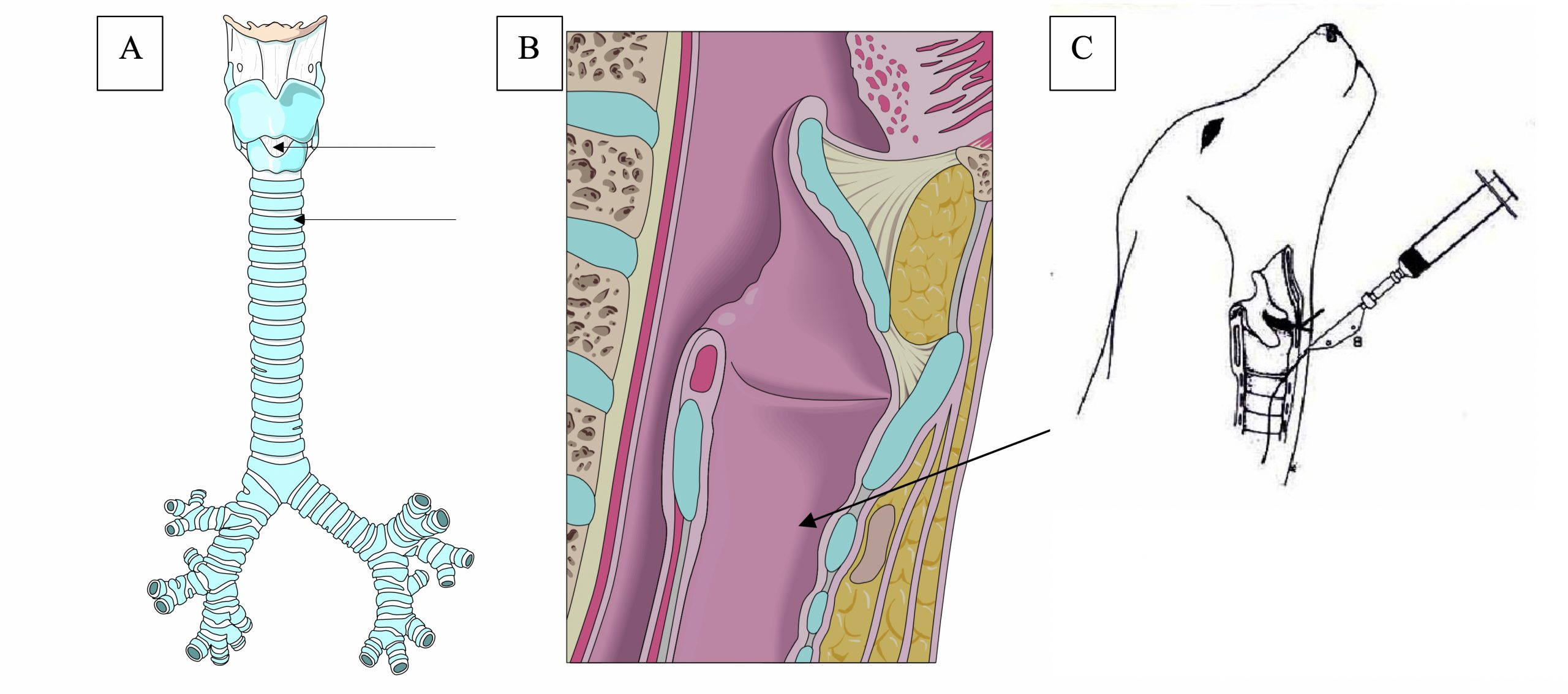
- Cricothyroid ligament: palpate up the ventral aspect of the trachea identifying tracheal rings. The first larger bump that is encountered is the cricoid cartilage. Immediately dorsocranial to this is a triangular depression, which is the cricothyroid ligament. Immediately dorsocranial to this depression is a second bump, which is the thyroid cartilage. The needle is placed into the cricothyroid ligament. If the needle is placed above the thyroid cartilage it will penetrate the epiglottis.
- Proximal tracheal rings: Identify the most ventrally palpable tracheal rings and identify the space between them. Usually only possible in larger dogs.

Video of TTW Procedure:
Details of TTW Procedure:
- Surgically prepare a 4-6 cm2 area over the chosen landmark (cricothyroid ligament or proximal tracheal rings).
- Inject 0.5 – 1.0 mL 2% lidocaine.
- Loosen connections on the through-the-needle catheter prior to removing the needle cover.
- Introduce the needle (bevel pointing down) through the cricothyroid ligament ORspace between the first few tracheal rings
- After puncturing the trachea, carefully redirect the needle ventrally to a 45o angle.
- Feed the catheter through the needle.
- Once the catheter is fully fed down the needle, seat the catheter firmly into the needle hub.
- Withdraw the needle from the trachea and skin so that it is just outside of the surface of the skin. Quickly apply the needle guard (requires firm pressure to close).
- Remove the stylet from the catheter.
- Attach a syringe filled with sterile saline to the catheter. Infusion volumes are usually around 1 mL/kg (maximum 10 mL).
- Immediately re-aspirate using empty syringes to retrieve your sample. Alternatively, if available, use a surgical suction unit connected to the needle hub for aspiration instead of using a syringe. Continuous suction is provided this way.
- An assistant should coupage the dog during suction, increasing the likelihood of productive coughing.
- Note that the volume retrieved is low in comparison to the amount infused. (Also note that in this lab retrieval will be minimal since there is no cough reflex.)
- If needed, 1-2 more aliquots can be infused, if the first aliquot did not yield a sufficient sample.
- Apply a bandage over the puncture site to minimize development of subcutaneous emphysema and pneumomediastinum.
Variation:
A tracheal wash can be performed in an anesthetized patient with an endotracheal tube in place:
- A sterile catheter or feeding tube can be pre-measured from the entry of the endotracheal tube to the approximate desired location (mid to distal trachea, estimated to be cranial to the xyphoid process.
- The tube is inserted via the endotracheal tube into the airway and advanced to the desired landmark.
- Aliquots of saline are infused, then retrieved from the sterile feeding tube. This technique is low-yield, meaning a very small sample will only be retrieved.