Understanding Normal and Abnormal Heart Sounds
Learning Objectives: Heart Sounds
- Describe what S1 and S2 are in relation to heart sounds
- Use proper stethoscope positioning and relevant anatomy to detect normal heart sounds
- Begin to develop familiarity with normal and abnormal heart and lung sounds
- Understand basic physiology of abnormal heart and lung sounds
- Listen to provided sound clips on Courselink to be introduced to normal versus abnormal heart sounds (murmurs or varying intensities, arrhythmias)
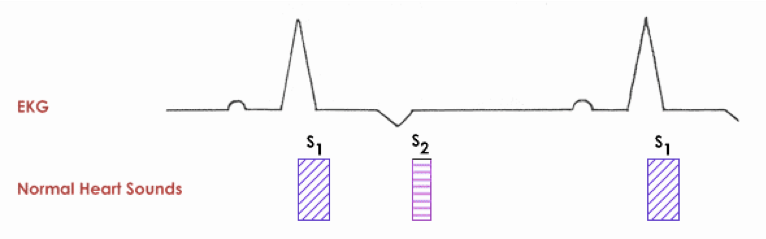
Normal Heart Sounds (S1 and S2)
First heart sound, S1:
- High frequency sound
- Heard best over the left apex
- With respect to timing: is associated with closure of the AV valves. This sound signals the onset of systole and correlates in timing with the QRS of the accompanying ECG.
Second heart sound, S2:
- High frequency sound
- Heard best over the left base
- With respect to timing: is associated with closure of the semilunar valves. This sound signals the end of ventricular ejection and occurs corresponding to after the end of the T wave on an accompanying ECG.
Third and fourth heart sounds, S3 and S4:
- It is difficult to distinguish between S3 and S4 in small animals
- If there is an extra heart sound in addition to S1 and S2, it is abnormal and often a gallop sound (see below).
Cardiac Murmurs:
- Heart murmurs are abnormal, extra sounds that are of a relatively long duration.
- Heart murmurs occur as a result of turbulence within the heart created by disturbed blood flow.
- Blood flow turbulence can be created by high-velocity flow, flow from a narrow region into a larger area, or low blood viscosity.
Causes of turbulence associated with heart disease:
- Valvular insufficiency (leakage)
- Valvular stenosis (narrowing)
- Connections between the cardiac chambers (i.e. interatrial and interventricular defects; holes)
- Connections between the great vessels (i.e. patent ductus arteriosus, PDA)
Are murmurs always due to cardiac disease?
Not always; A few examples of murmurs existing without cardiac disease:
Functional or physiologic murmurs can be associated with low blood viscosity (anemia, hypoproteinemia) instead of actual cardiac disease. These murmurs are usually low grade (< grade 3). In contrast, note that if blood viscosity is increased, a murmur may be masked.
Young animals (< 6 months of age) can have functional heart murmurs in absence of cardiac disease in other situations. These murmurs should resolve by 6 months of age, and tend to have the following characteristics:
- Soft, low intensity sounds (grade 1/6 to 2/6)
- Occur early in systole
- PMI over the left base
- Tend to vary in intensity with a change in HR or body position
- These are important features to distinguish innocent murmurs from congenital heart murmurs.
Other functional murmurs can be present in athletes, and in pathologic states such as fever, anemia, or hypoproteinemia.
Anything that muffles the heart sounds can obscure a murmur such as obesity, thoracic effusions, or loud respiratory sounds.
Point of Maximal Intensity (PMI):
A presumptive diagnosis is usually possible based primarily on the timing of the heart murmur, and the point of maximal intensity (PMI) of the murmur. In Clinical Medicine I, goals are to practice ausculting over the PMI for each valve.
The PMI refers to the location where the murmur is loudest.
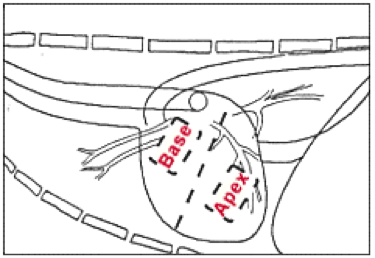
The left chest wall is typically divided with respect to PMI into two positions.
- Left heart base (includes both the pulmonic valve and aortic valve areas, and discriminating between these two is often problematic in small animals)
- Left heart apex (over the mitral valve)
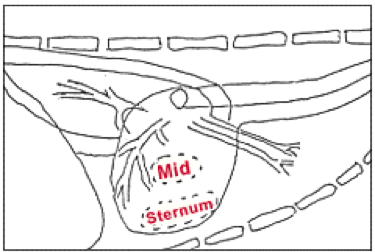
The right chest wall is typically divided with respect to PMI into two positions:
- Mid heart (over the tricuspid valve)
- Sternal border (typical location of VSD murmurs)
Grading of murmurs is often performed on a 1-6 scale (for systolic murmurs, the most common type we encounter clinically). When ausculting a murmur, compare its intensity to the intensity of the normal heart sound.
- Grade 1: Very soft, difficult to detect
- Grade 2: Soft, less intense than normal heart sound
- Grade 3: Same intensity as normal heart sound
- Grade 4: Moderately louder than normal heart sound
- Grade 5: Loud, accompanied by precordial thrill over PMI
- Grade 6: Very loud, accompanied by precordial thrill over PMI, murmur detected when stethoscope slightly off of chest wall.
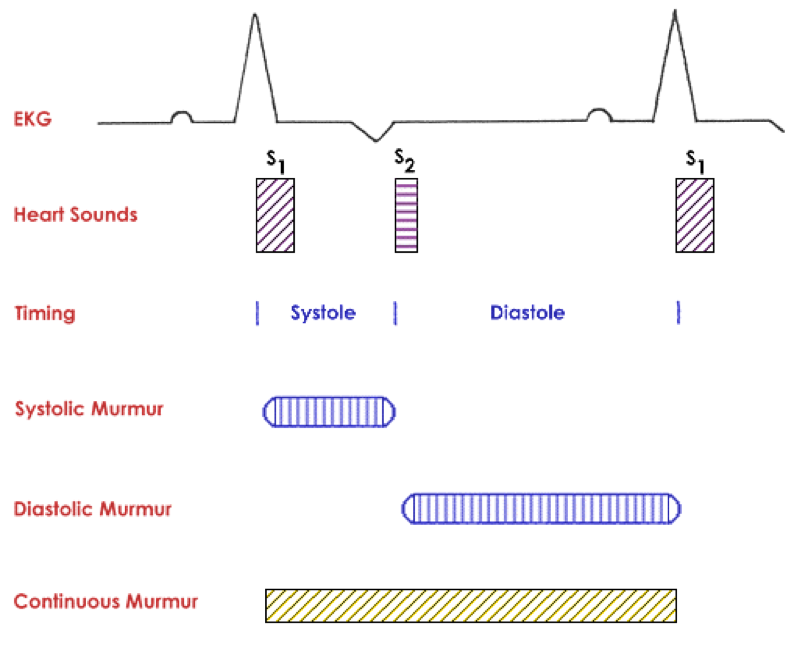
Timing of murmurs, at the PMI, is generally divided into one of three classes:
- Systolic (occurring during systole)
- Diastolic (occurring during diastole)
- Continuous (present at all times)
Systolic murmurs:
- The very vast majority of murmurs are systolic
- When soft they are usually early in systole and disturb the end of S1. S1 often appears slurred in these cases as opposed to ending abruptly as is normally the case.
Diastolic murmurs:
- Very rare
- Low frequency
- Rather low intensity and so are graded out of 4, not 6
- Best identified with the bell of the stethoscope
Continuous murmurs:
- Common
- Typically associated with a PDA, but also arteriovenous fistulas
- Usually vary in intensity throughout the cardiac cycle, however the murmur is detected at all times
- The continuous nature of the murmur may only be noted at the PMI, while at other locations it may only be systolic, for example.
These concepts will be explored in further detail later in the DVM curriculum.
Notes on feline cardiac murmurs:
- In the cat, the areas of typical location for murmurs in dogs are not useful. Murmurs are typically loudest located along the sternum or just off the right or left side of the sternum. Murmurs can be located in the caudal part of the thorax or cranial part of the thorax in the cat.
- About 20-25% of murmurs in cats are not associated with any substantial pathology.
- Gallop sounds may be normal in older stressed cats.
